Roswell Park offers several options for removing large or difficult colon and rectal polyps — without surgery.
The rates for colorectal cancer have decreased dramatically ever since colonoscopy became the gold standard for colorectal cancer screening. Colonoscopy not only detects early signs of cancer — in the form of small growths called polyps — but the procedure can also remove any polyps before they become cancerous, preventing colorectal cancer from ever developing.
However, some polyps found during screening colonoscopies cannot safely be removed during the procedure. These so-called complex polyps are considered difficult, because they are either too large, too flat, or located in an area that makes them unsuitable for conventional removal.
For these patients, Roswell Park Comprehensive Cancer Center has created a new program — Complex Polypectomy Program — that allows their highly trained gastroenterologists and colorectal surgeons, with the aid of advanced devices and technologies, to deliver nonsurgical, endoscopic treatment of these complex polyps.
What is a complex polyp?
The term complex polyp refers to a colon or rectal polyp that can be more challenging to remove than most polyps typically encountered on colonoscopy. Features of a complex polyp include:
- Large size (greater than 2 centimeters)
- Difficult-to-reach location
- Very flat shape
Complexity of a polyp can be in the eye of the beholder, but based on objective size alone, on average around 1% to 5% of polyps that are found are greater than 2 centimeters in dimension. In total, up to 15% of polyps are considered difficult.
By definition, all polyps are considered precancerous, or adenomas. In that sense, although they are benign or noncancerous at the time of identification, they run the risk of turning into cancer down the road.
Treatment options for complex polyps
Roswell Park offers several option to manage complex polyps. Some are nonsurgical approaches: endoscopic mucosal resection, endoscopic submucosal dissection or endoscopic full thickness resection. Sometimes surgical approaches, including robotic and/or transanal surgery, are indicated.
Generally, polyps in the innermost mucosa layer of the colon wall are treated with endoscopic mucosal resection. Polyps that have grown deeper, and into the submucosa layer, are treated with endoscopic submucosal dissection.
For the patient, these procedures similar to undergoing a colonoscopy. During the procedure, the physician locates the polyp and injects a cushion of fluid underneath it to “lift” it off of the colon wall. Then the polyp is removed with a snare. A repeat colonoscopy is typically performed in three to six months to reassess and confirm there is no residual tissue or regrowth.
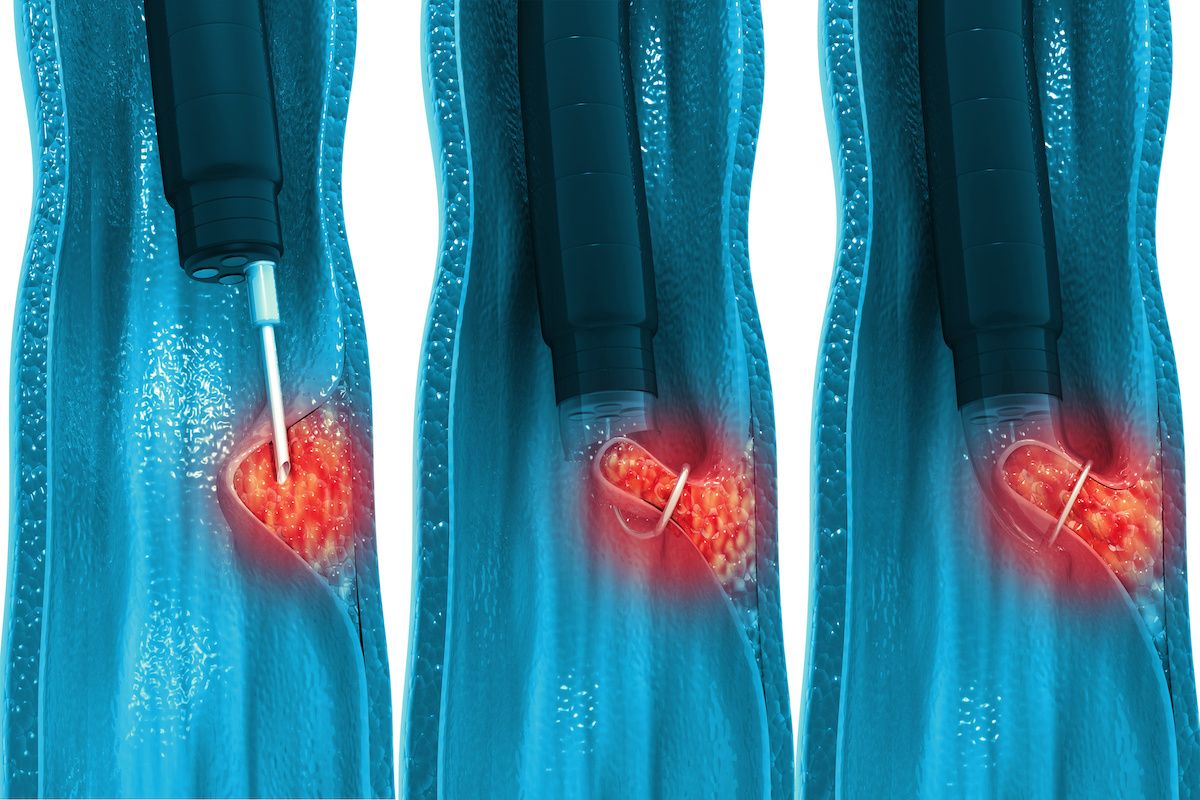
A procedure called endoscopic full thickness resection is performed for polyps located further in the wall of the colon or rectum. Your doctor will use forceps to pull the polyp away from the colon wall, and remove it with a special clip that remains in place to close the wound.
All of these complex colonoscopies are performed through the anus and without abdominal incisions. The majority of patients are sent home the same day, with minor limitations on activity for the rest of the day and may return to normal activity and diet the next day.
Know Your Risk
Roswell Park recommends that everyone at average risk begin regular colorectal cancer screening at age 45 — earlier if you have certain risk factors or family history.