

Surgery to remove the cancer during an operation is a primary treatment for stomach cancers. It is essential that you seek a surgeon who is highly experienced in performing the type of surgery that you need.
The National Comprehensive Cancer Network (NCCN) advises patients to seek care from a high-volume center that performs 15 to 20 stomach surgeries each year. Roswell Park’s gastrointestinal surgeons – who focus on surgery specifically for cancer – perform 60 to 70 of these surgeries each year.
The type of surgery you may need may include one of the following procedures:
- Endoscopic resection. Some early-stage cancers may be removed from the stomach without any actual incisions. Using the endoscope (thin, flexible tube) passed through the throat, your physician can suction or cut away the lesion or tumor. This approach is an option for small (2 centimeters or less) tumors that have not grown beyond the first layer of the stomach wall. Roswell Park offer two types of endoscopic resection procedures, including:
- Endoscopic mucosal resection (EMR)
- Endoscopic submucosal dissection (ESD)
- Gastrectomy. This operation removes part (called resection) or all of the stomach. During a gastrectomy, the surgeon will also remove lymph nodes (typically at least 30) from the area to examine them for cancer. Your physician team will determine which type of gastrectomy is right for treating your cancer. These include:
- Total gastrectomy which removes the entire stomach, nearby lymph nodes and parts of the esophagus and small intestine. The esophagus is then reconnected to the small intestine.
- Partial (subtotal) gastrectomy removes only the portion of the stomach that contains the cancer, nearby lymph nodes and sometimes part of other nearby organs.
- Proximal gastrectomy for tumors at the gastroesophageal junction (where the esophagus meets the stomach). This operation removes the about half of the stomach, the GE junction and a few centimeters of the esophagus. The esophagus may be reconnected to the stomach, or a piece of small intestine is used between the stomach and the esophagus to minimize reflux. A newer double-tract reconstruction technique results in fewer long term side effects and better quality of life.
- Gastrojejunostomy is an operation that may be performed when a tumor blocks the small intestine. A gastrojejunostomy creates an alternate pathway for food to get from the stomach to the small intestine.
Novel approaches for tumors in difficult locations

Our highly experienced surgeons perform unique surgical options that spare more of the stomach and/or reconstruct key structures for optimal function and quality of life. These include:
- Intragastric surgery. This procedure uses small incisions and ports placed on and inside the stomach to remove tumors in tough locations, especially where the esophagus and stomach meet. This obviates the need to remove large portions of the stomach especially the sphincter that lies at the junction of esophagus and stomach.
- Double tract reconstruction after proximal gastrectomy. This is a technique for cancer near or at the gastroesophageal junction, meaning more of the stomach can be preserved and the esophagus is reconnected to both the stomach and the small intestine. This minimizes the incidence of reflux associated with the procedure.
- Jejunal Pouch creation after total gastrectomy. For patients that need the entire stomach removed, surgeons use the small intestine to construct a jejunal pouch which acts as a reservoir so patients can tolerate a larger meal, avoid excessive weight loss and enjoy better quality of life.
We can offer a minimally invasive, small incision approach to more than 90% of our patients and we perform a high volume of these with excellent outcomes.
What is robotic surgery?
Robotic surgery is a minimally invasive technique in which surgeons operate through a few tiny “keyhole” incisions in the abdomen, aided by a tiny lighted camera inserted through one incision, to provide a magnified view of the operating field. Robotic instruments are inserted through these keyholes and controlled by the surgeon. This provides superior 3D visualization, improved dexterity and more degrees of mobility, which allows the surgeon to perform surgery with more precision. The stomach is very accessible with these tools, and compared to traditional open surgery, robot-assisted procedures are associated with:
- Reduced hospital stay
- Fewer wound infections
- Less pain
- Less blood loss
- Faster recovery
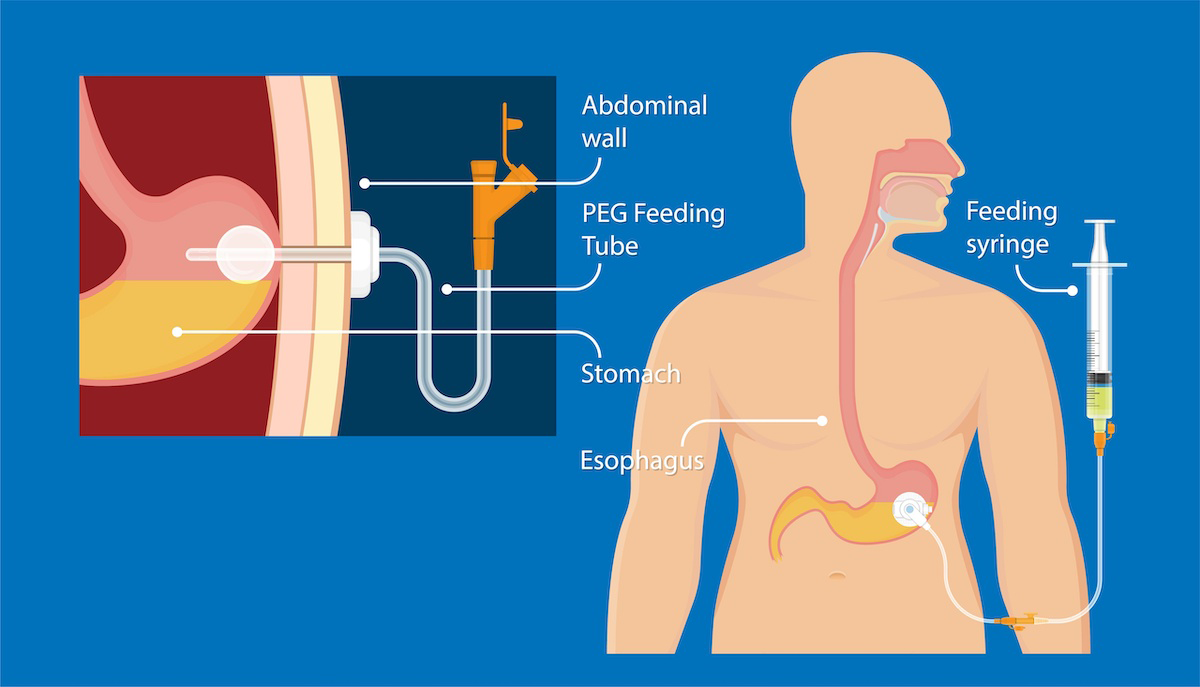
Will I need a feeding tube?
As part of their surgery, some patients will have a soft, plastic tube placed through the skin of their abdomen and directly into the stomach, called a gastrostomy tube (G-tube) or into the small intestine, called a jejunostomy tube (J-tube). These temporary tubes can deliver food and medicine as you heal from the surgery and you’re able to get enough nutrition eating by mouth.